
Medical Considerations
Abortion has been observed in many species as a response to severe physiological stress. Starvation may result in abortion as a protective mechanism to conserve the maternal animal’s own body reserves. Stresses associated with transport, close housing, sudden reduction or change in food and water intake, and other debilitating factors will cause abortion in pregnant mares, especially during the middle of pregnancy (Roberts, 1980). Miller (1980) notes that abortion in emaciated cattle may occur, but that abortion or premature delivery in these cases does not preserve the life of the anima1. Rather, it heralds a terminal event. The report recommends the induction of parturition at an earlier stage in these animals.
Glucocorticoids administered in repeated doses over several days have been used to stimulate abortion in the last trimester of pregnancy in horses (Roberts, 1980). In contrast, similar treatments have no effect on the termination of pregnancy in many other species. Administration of exogenous adrenocorticotrophin (ACTH) or corticosteroids can disrupt implantation and fetal development in sheep and rats. Currently, it is difficult to predict the concentration of adrenal hormones released during a specific stressful event, and whether the levels would be sufficient to result in abortion (Moberg, 1985).
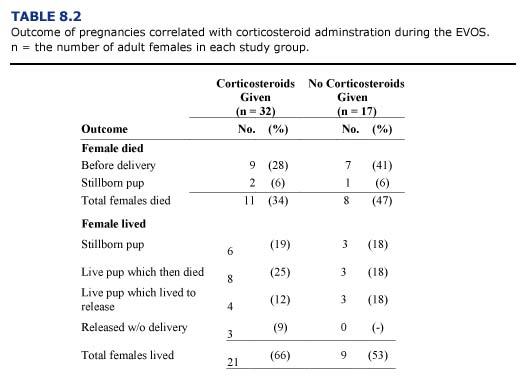
Several forms of glucocorticoids (dexamethasone, prednisolone, triamcinolone) were routinely used to combat shock in debilitated sea otters during the EVOS. Use of these drugs in females was discontinued after it was suspected that corticosteroids contributed to the high incidence of abortion and stillbirths in the centers. To evaluate this, we compared the outcome of pregnancies for otters receiving and not receiving steroids during rehabilitation (Table 8.2). The total number of otters in this study was relatively small and many other variables influenced the condition of the pregnant animals. In general, survival rates were comparatively better for females receiving corticosteroids at admission. The rates of stillbirths and neonatal deaths were similar for both groups. Based on these results, corticosteroid administration should be considered.
During the EVOS, live pups were taken from twelve females which were unable to care for them during the first few hours after birth. Most of these neonates were never able to nurse and were hypothermic due to the inability of the mother to keep the pup’s fur properly groomed. Newborn pups are susceptible to chilling and may drown or be injured if the female is inattentive. Pups which become hypothermic due to poor grooming or immersion in water are very difficult to stabilize. Only one of the pups removed from its mother survived. It was transferred to Point Defiance Zoo and Aquarium where it died at about four months of age. The poor viability of pups born to debilitated otters at the centers is not surprising, but the effect of oil exposure, capture stress, medical treatments, husbandry techniques, and natural maternal abilities on survival remain uncertain. Although maternal survivorship dramatically improved once the oil weathered, the mortality in the offspring remained high. Viable pups were not delivered in the rehabilitation centers until nine weeks after the oil spill. Fifty percent of the deliveries after this period still resulted in death of the offspring, although no further maternal deaths occurred.
Dystocia (delayed or difficult delivery of a full term fetus) is a potential problem in a rehabilitation center. At least two sea otters treated during the EVOS experienced difficult labor. Oxytocin and calcium injections were administered to one of these females in an effort to strengthen contractions, but the effect was questionable. Both otters eventually delivered very large, stillborn pups following more than twenty-four hours of labor. The untreated female subsequently developed a purulent vaginal discharge and was given antibiotic injections for several days before making a full recovery. A captive sea otter housed for more than two years in a seaquarium had to be assisted with the delivery of a large, stillborn fetus after several hours of unproductive effort. This otter sustained pelvic trauma which resulted in paralysis; death occurred several days later (Vancouver Aquarium Animal Care Department, personal communication). Cesarean section may be performed using fentanyl/diazepam sedation and standard surgical procedures if dystocia is determined to be life threatening.
Uterine torsion has not been reported as a cause of mortality in wild sea otters but has been observed and surgically corrected in an otter housed in a seaquarium (T. D. Williams, Monterey Bay Aquarium; personal communication). The high incidence of uterine torsion observed during the EVOS was a definite concern. The weight of the gravid uterus may not be properly supported when the otter is out of water; transport for prolonged periods in kennel cages while the otter struggles may result in torsion. Excessive rolling and violent activity during capture or while under sedation may also predispose the female to this condition. Female otters in advanced pregnancy should be moved with care and observed closely for signs of abdominal distress. Early surgical intervention is required for correction once torsion has occurred. Prevention or early detection is important.