An initial clinical examination is required to determine if the animal should be:
1) released untreated,
2) cleaned of oil and released,
3) cleaned of oil, treated, and released, or
4) cleaned of oil and held in captivity for long-term treatment.
All animals should be temporarily marked, preferably with a color coded tag that identifies what level of attention they may need. Flipper tags (e.g. Jumbo rototags; Dalton-supplies, Heneley-on-Thames, England) are effective. Assessment should then address the following general categories, which were found to be useful in dealing with oiled New Zealand fur seals (Gales, 1991).
Degree of Oiling
An arbitrary scale of 0-5 may be used, where 0 represents no contamination and 5 represents complete coverage with oil.
Mass
This is used as an approximate index of nutritional status. Unlike sea otters, which have a high metabolic rate and depend on regular caloric intake (Costa and Kooyman, 1982), pinnipeds are physiologically capable of fasting. Thus, acute metabolic dysfunction such as hypoglycemia (Chapter 5) is less likely in pinnipeds. A reduced or zero caloric intake is manifested primarily as a decrease in mass in pinnipeds.
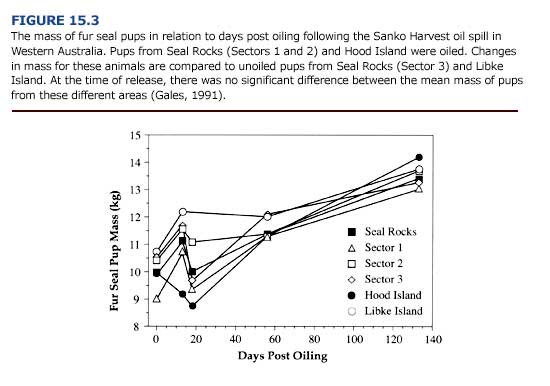
Measurement of mass is probably only practical in small pinnipeds. For larger animals, condition indices such as ultrasonic measurement of blubber thickness can be used. Mass can also be used to quantify recovery. Davis and Anderson (1976) demonstrated a decreased growth rate and a lower average peak mass for oiled gray seal pups compared with unoiled pups. Gales (1991) showed that oiled fur seal pups underwent a marked decrease in mass following the oiling event, but recovered to normal levels in 140 days (Figure 15.3).
Clinical Signs
Hypothermia and/ or stress due to toxicosis can be recognized by shivering and a moribund or even comatose state. Core body temperature should be measured with a digital thermometer with a flexible probe. However, it is unlikely that core temperature will be as labile in pinnipeds and polar bears as it is in oiled sea otters. Respiratory injury, such as the interstitial emphysema reported for oiled sea otters (Chapter 5), has not been reported in pinnipeds. This may reflect a lack of sufficient monitoring of oil exposed pinnipeds, or a possible higher tolerance to pulmonary contact with petroleum hydrocarbons. Emphysema was recorded for one polar bear following experimental exposure to oil (0ritsland et al., 1981).
Dehydration is commonly observed in oiled wildlife. The degree of dehydration can be roughly assessed using a skin pinch test. In dehydrated seals and polar bears, the skin will remain raised for several seconds after pinching. This test is not definitive and is less appropriate for thick skinned pinnipeds with abundant subcutaneous blubber. Hematology can provide a more accurate measure of fluid balance. The degree to which an animal avoids capture and resists handling is also a good index of clinical state. Surface contact of oil on eyes and mucous membranes should be noted.
Treatment is initially based on clinical signs, and later on of clinical pathology results (see below). Irrigating eye washes and broad spectrum ophthalmic antibiotics should be used to treat eye injuries. Systemic fluid treatment administered subcutaneously or orally may be used when indicated. Ringer’s solution is appropriate for subcutaneous injection. Dextrose administration is only indicated in hypoglycemic animals.

